
I. Gynecologic Cancer In Indonesia


II. The Initial Management Of Ovarian Cancer The treatment of ovarian carcinoma is multidisciplinary in nature. Chemotherapy has had a major impact on survival and, currently, most patients receive platinum-containing combinations3,4.The Treatment Of Ovarian Cancer are there should be accepted treatment for patients with recognised disease—The surgical management of women with an ovarian malignancy is well established and chemotherapeutic agents are used as adjuvant treatment if extra-ovarian spread is identified. The vast majority of patients with stage Ia or Ib ovarian cancer have an extremely good prognosis following surgery alone. The facilities for diagnosis and treatment should be available— The two most extensively investigated diagnostic methods used for ovarian cancer screening, the tumour marker CA 125 and real-time ultrasonography, are now routinely available to most practitioners throughout the developed world. Transvaginal probes can be added to standard equipment used for other purposes. Surgical and chemotherapeutic facilities for treatment of ovarian cancer are widely available whether in specialist centres or general hospitals.5,7
III. The Malignancy Risk Index


Ovarian cancer is the leading cause of death from gynecologic cancer in women. Surgery plays a key role in the management of the disease, and it is important for making the diagnosis, identifying prognostic factors, alleviating symptoms and extending survival. Unfortunately, there is evidence that some women are not being appropriately staged or optimally debulked at the time of initial surgery. In addition to having a direct impact on survival, inadequate initial surgical management can result in greater morbidity because of a need for repeat abdominal surgery1,2,4.
In 2002, reported marked differences in staging and debulking as a result of the surgical management of incident ovarian cancer in Ontario depending on the specialization of the surgeon and hospital. We also demonstrated a volume–outcomes effect in which repeat surgery was more common among patients who underwent initial surgery in institutions with low surgical volumes where no gynecologic oncologist (GO) was present or where the initial surgery was performed by someone other than a GO. We also found that patient survival varied depending on the discipline of the surgeon who performed the initial procedure. Patients with ovarian carcinoma have the worst prognosis of all patients with gynecologic malignancies. Their overall 5-year survival rate approximates 40%, mainly due to the large proportion of patients who present with advanced disease. The life-time risk of developing ovarian carcinoma is 1 in 75.3,4
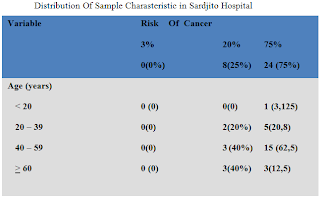
The total number of new cancer cases in 1994 from 12 cancer registries, based on pathological reports, was 23.310 ( 8459 males and 14.820 females). The most common cancer sites in males were colon-rectum (1002 cases), nasopharynx ( 856), skin (833), soft tissue (501 ), prostate gland ( 449 ), and in females they were cervix ( 4126 cases), breast (2743), ovary (1200), colon rectum ( 902 ) and skin (831). Department of Health assumes cancer incidence to be 100 per 100,000 people. Based on pathology, there were 10 most frequent cancer in male and female together i.e. cancer of the cervix, breast cancer, skin, rectum, nasopharynx, ovary, lymph nodes, colon, thyroid, and soft tissue. Cancer of the cervix also appears as the most frequent cancer among female, and its position was the first rank, followed by breast, ovary, skin, thyroid, rectum, lymph nodes, uterus, colon, nasopharynx.1,2 There were slight differences between pathological and hospital- based data (Table 2). Cancer of the cervix was about 75% among gynecological cancer and they were mostly diagnosed at advanced stages (Table 3).7,8,9


During the initial management of ovarian cancer, it is crucial that appropriate and high-quality surgical procedures be performed to obtain correct staging information, achieve optimal cytoreduction, and guide decisions about subsequent therapy. However, there is evidence that the recommended surgery for ovarian cancer is often not performed. Several studies, found that more highly specialized surgeons (i.e., gynecologic oncologists) were more likely than less-specialized surgeons (i.e., general surgeons) to perform the recommended surgery for ovarian cancer . Moreover, two studies have shown that 20 – 30% of ovarian cancer patients thought to have early-stage disease were found to have had more advanced-stage disease at a second surgery if the appropriate staging procedures were not performed at the first surgery5,6. Because of such observations, the National Institutes of Health (NIH), American College of Obstetricians and Gynecologists, and Society of Gynecologic Oncologists have recommended that all women with ovarian cancer except those suspected of having very early-stage cancer be referred to a gynecologi oncologist for the initial management of their disease.
Surgery is important to determine the correct disease stage and to remove as much tumor as possiblein patients. Several studies have shown that patients with ovarian carcinoma who underwent surgery by a gynecologist had better survival compared with patients who underwent surgery by a general surgeon9. Subsequently, it was suggested that surgery by a gynecologic oncologist would improve survival further.However, that hypothesis could not be confirmed in a large population-based study on differences in patterns of care of patients with ovarian carcinoma.10 In a more recent population-based study on the impact of surgery by a gynecologic oncologist compared with a general gynecologist, a survival benefit was found for patients with International Federation of Gynecology and Obstetrics (FIGO) Stage III disease. were included in the study population, and the effect of treatment in teaching hospitals was not addressed.,7,8,9 However, because it also was found that gynecologic oncologists attained optimal cytoreduction more often compared with general gynecologists, it is expected that survival will be improved when surgery is performed by gynecologic oncologists1,2
The screening test of ovarian cancer there should be a suitable test or examination—Both high sensitivity (the probability of the test being positive in individuals with the disease) and high specificity (the probability of the test being negative in individuals without the disease) are important requirements for a screening test. Unfortunately, an increase in the sensitivity of a test often results in a reduction in specificity and vice versa. In ovarian cancer screening the outcome of a positive test will be a diagnostic surgical procedure and neither patients nor clinicians will accept large numbers of operations for each case of cancer detected. Therefore, specificity is a major consideration when deciding on which test to use for screening8.
A variety of modalities have been used to detect ovarian cancer in asymptomatic women4,5:
1. Vaginal examination
Several studies have investigated the use of vaginal examination in ovarian cancer screening and all of them have shown that the specificity of this method is insufficient
for use as a first-line screening tool in asymptomatic women.
2. Tumour markers
Non-invasive tests are the most likely to be acceptable to individuals participating in a screening programme and therefore many tumour markers for ovarian cancer have been investigated. Serum levels of oncofetal proteins such as carcinoembryonic antigen (CEA) and alpha- fetoprotein, as well as antigens defined by monoclonal and polyclonal antisera have been assessed as markers for epithelial ovarian cancer. Enzymes, hormones and metabolic products have also been studied. However, the only tumour marker to have been studied prospectively is CA 125 and the results of retrospective analyses of other markers cannot be extrapolated to screening asymptomatic women with any confidence. CA 125, an antigenic determinant on a high molecular weight glycoprotein recognised by a mouse monoclonal antibody (OC 125) developed using an ovarian cancer
3. Ultrasound
Ultrasonographic assessment of the ovaries has been extensively investigated. Transabdominal ultrasound examination, when evaluated prospectively in 5540 women had a high false positive rate (5.4%). Many of the false positive cases had benign or functional ovarian cysts, but 25.7% of the false positives had no ovarian pathology at diagnostic operation. It is difficult to distinguish between benign or functional ovarian masses and malignant tumours using transabdominal ultrasound, but transvaginal scanning offers greater resolution and has improved the quality of ovarian morphological assessment.
4. Other modalities
Other imaging methods used in the assessment of clinically detected ovarian masses such as computed tomography (CT), magnetic resonance imaging and radioimmunoscintigraphy cannot be advocated for screening purposes due to their cost and availability as well as patient acceptability and, in the case of CT, radiation exposure. However, they may have an important role as tertiary tests.
The prevalence of ovarian malignant neoplasm has been rising in the last 30 to 40 years. Since its occurrence and development is very latent, and since there have been few effective tools for early diagnosis and treatment, its mortality rate has been the highest among gynecologic malignant neoplasms2,3. If ovarian carcinoma patients can be diagnosed at Stage I, the cure rate could be as high as 80% to 90% and the mortality could decrease a half. So a new method of early diagnosis would have great significance for prediction of the prognosis and treatment of ovarian neoplasms. The positive rate of preoperative diagnosis of ovarian malignant neoplasm in Stages I, II and III by serum CA125 level can be as high as 50% and 80% to 90%, respectively. In borderline tumors, the preoperative positive rate for Stage I was 40%, and for Stages II-IV, 90%-100%. But CA125 alone has limited clinical use for detecting some ovarian benign neoplasms or mucinous carcinomas. In contrast, the ultrasound score system plays some role in preoperative prediction of ovarian benign or malignant neoplasm. In our study, the ultrasound score system (cutoff value ≥2) had a sensitivity of 94%, a specificity of 83%, and a positive predictive value of 82%. However, using the ultrasound score alone produced slightly more false positives7,8,9.
RMI is the integration of serum CA125 level, menopausal status and ultrasound findings. This overcomes the false-positive problem found in using single factor alone, and increases the sensitivity and specificity in the preoperative diagnosis of ovarian malignant neoplasm. In the preoperative diagnosis of ovarian malignant neoplasm, RMI has higher sensitivity and positive predictive value than CA125 at the similar specificity, so it has offered a new way to diagnose an ovarian mass. In the standard curve of successive RMI, and RMI of over 200 can be known to have a sensitivity of 87.3% and specificity of 84.4%7,8. These results are similar with those of Tingulstad. Ovarian neoplasms in Stage III or IV was much more (73%) prevalent than the ovarian malignant neoplasm. This was the main reason that the sensitivity of RMI in our study in prediction of pelvic malignant neoplasm was higher than that of other authors'9.
Advice of application on RMI. Most benign neoplasm patients and a few malignant neoplasm patients have low RMI scores. In the 63 cases of malignant neoplasm, RMI of seven cases (11.1%) was less than 200. Among these low-scoring cases, there were four cases of granular cell tumors, one case of mucinous cystadenocarcinoma, one case of Setoli cell tumor and one case of borderline tumor8,9. As CA125 has limited value in recognizing mucous carcinomas, it led to low RMI scores, and therefore should always be analyzed in combination with the ultrasound findings. There were four cases of RMI <200 in the six cases of granular cell tumors, and their overall level of RMI was relatively low. In this respect, they resembled borderline tumors, but presented low malignant potential. Therefore it was difficult to diagnose by RMI, and preoperative diagnosis in such cases should take into consideration the history of the endocrine change for greater accuracy.
Serum CA125 in patients with endometrioma and pelvic inflammatory cysts is often very high since it is mainly associated with anti-CA125 antibody in the active mesothelial tissue of peritoneum and inflammatory tissue. Such high. levels of CA125 can greatly increase the RMI. In our study, serum CA125 in patients with endometrioma and pelvic inflammatory cyst was consistently higher than that of patients with other benign masses. However, compared with the increase of RMI in malignant neoplasm, it increased a little.. Those patients were often young, so correct preoperative diagnosis could best be made with RMI, history and carefully physical examination in concert3,4,5.
Many serum markers such as CA125, alpha-fetoprotein, human chorionic gonadotrophin and lactate dehydrogenases. as well as ultrasound techniques',have been proposed to enable differential diagnosis of benign and malignant ovarian masses. Ultrasonographic investigation of ovarian masses by the transabdominal or transvaginal routes enables quite accurate evaluation of the characteristics of the mass (sensitivity62%-100%)6,7. However since the specificity of the method is only 73%-95%, it is not possible to predict with certainty whether the mass is benign or malignant'. To increase the capacity of ultrasonographic investigation to predict the malignant potential of an ovarian mass, many scoring systems have been developed for objective evaluation of changes in morphological parameters (volume, internal echogenicity, the nature of the walls, the presence of septa, papillae and solid parts). The application of this scoring system has certainly improved the specificity of the method, but it has not reduced the number of false positives7.
Various combined methods of evaluating the risk of ovarian cancer in women have been proposed. Two scoring methods based on menopausal status, ultrasonographic examination and serum concentrations of CA125, have given much better results than single determinations, with the advantage of being practicable even in less specialised gynaecology clinics. The risk of malignancy index (RMI) is calculated with a simplified regression equation obtained from the product of the ultrasonographic investigation score (U), the menopause score (M) and the absolute value of serum CA125. The RMI developed by Jacobs et ~ 1 .is’ ~ known as RMI 1, whereas that developed by Tingulstad et al is known as RMI 2 and has only been used in a single population, namely the one from which it was derived. The difference between the two indices lies in the different evaluation of U and M8,9.
A score was assigned for ultrasound investigation characteristics: the presence of multilocular cystic lesions, solid areas, bilateral lesions, ascites and intra-abdominal metastates, scored one point each. A total ultrasound score (U-score) was calculated for each patient. Postmenopausal status was defined as one year or more of amenorrhea, or an age of 50 years or more if the woman had undergone hysterectomy.
RMI 1 and RMI 2 were calculated for all patients together with the sensitivity, specificity and positive and negative predictive values of the two methods. RMI 1 (Jacobs et al.) = U x M x serum CA125, where a total ultrasound score of 0 gave U = 0, a score of 1 gave U = 1 and a score of > 2 gave U = 3; premenopausal status gave M = 1, postmenopausal M = 3. The serum level of CA125 was multiplied directly into the formula. RMI 2 (Tingulstad et al.) = U x M x serum CA125, where a total ultrasound score of 0 or 1 gave U = 1 and a score of > 2 gave U = 4; premenopausal status gave M = 1, postmenopausal M = 4; the serum CA125 concentration was substituted directly into the formula. 7,8,9




III. Conclusion
In conclusion, the risk-of- malignancy index is apparently able to identify the probability of malignant pelvic masses, by incorporating serum CA 125 serum levels, ultrasound morphology and menopausal status, performed individually in women with ovarian masses. The main purpose of this study was the evaluation of a risk-of-malignancy index defined in a selected population of apparently early lesions. This index is a simple score system which can be applied directly to clinical practice and might be of value in the preoperative assessment of the adnexal mass. It showed it self useful in referring patients with advanced neoplasia to a more complex healthcare unit, although it does not seem to show prognostic value. However, the performance of the present index must be evaluated in other studies, using a validation sample from a similar population.
As opposed to other strategies for preoperative discrimination of pelvic masses,12–15 the risk-of-malignancy index can be applied directly to daily clinical practice without establishing expensive, laborious, and complicated new methods. The simplicity and applicability of the method remains to be seen whether centralization will actually improve survival and quality of life for these women.
Daftar Pustaka
- Sarjadi, Padmi Trihartini Cancer Registration In Indonesia, Asian Pacific Journal of Cancer Prevention, Vol 2, 21-24 IACR Supplement, 2001
- M. Farid Aziz, Gynecological cancer in Indonesia, J Gynecol Oncol Vol. 20, No. 1:8-10, March 2009 DOI:10.3802/jgo.2009.20.1.8
- Laurie M. Elit, MD;* Susan J. Bondy, PhD;†‡ Lawrence P. Paszat, MD et al, Surgical Outcomes in woman with ovarian cancer J can chir, Vol. 51, No 5, octobre 2008
- Craig C. Earle , Deborah Schrag , Bridget A. Neville , K. Robin Yabroff, et al,effect of surgeon speciality on processes of care and outcomes for ovarian cancer patients, Journal of the National Cancer Institute, Vol. 98, No. 3, February 1, 2006
- Mirjan J.A. Engelen, MD. Henrike E. Kos, M.Sc et al, surgery by consultant gynecologic oncologist improves survival in patients with ovarian, Published online 20 December 2005 in Wiley InterScience
- Giuseppe Morgante Consultant, Antonio la Marca Resident, Antonino Ditto Resident et al, Comparison of two malignancy risk indices based on serum CA 125, ultrasound score and menopausal status in the diagnosis of ovarian massesJune 1999, Vol106, pp. 524-527 RCOG 1999 British Journal of Obstetrics and Gynaecology
- CarolineVanHolsbeke,1,4Ben VanCalster,3 Lil Valentin,7AntoniaC.Testa et.al, External validation of mathematical Models to distinguish Between benign and Malignant Adnexal Tumours : A multicenter study by the International Ovarian Tumour Analysis GroupClin Cancer Res 2007;13(15) August1, 2007
- Amer Raza, MRCOG,* Tim Mould, MRCOG,Þ Meg Wilson, MRCOG, Increasing The effectiveness of referral Of Ovarian Masses from cancer unit to cancer center by using a higher referral value of the risk of malignancy index International Journal of Gynecological Cancer & Volume 20, Number 4, May 2010

Tidak ada komentar:
Posting Komentar